
Cancers that are known collectively as head and neck cancers usually begin in the squamous cells that line the moist, mucosal surfaces inside the head and neck (for example, inside the mouth, the nose, and the throat). These squamous cell cancers are often referred to as squamous cell carcinoma. Head and neck cancers can also begin in the salivary glands, but salivary gland cancers are relatively uncommon. Salivary glands contain many different types of cells that can become cancerous, so there are many different types of salivary gland cancer.
Cancers of the head and neck are further categorized by the area of the head or neck in which they begin. These areas are described below and labeled in the image of head and neck cancer regions.
Includes the lips, the front two-thirds of the tongue, the gums, the lining inside the cheeks and lips, the floor (bottom) of the mouth under the tongue, the hard palate (bony top of the mouth), and the small area of the gum behind the wisdom teeth.
The pharynx (throat) is a hollow tube about 6 inches long that starts behind the nose and leads to the esophagus. It has three parts: the nasopharynx (the upper part of the pharynx, behind the nose); the oropharynx (the middle part of the pharynx, including the soft palate [the back of the mouth], the base of the tongue, and the tonsils. And the hypopharynx (the lower part of the pharynx).
The larynx, also called the voicebox, is a short passageway formed by cartilage just below the pharynx in the neck. The larynx contains the vocal cords. It also has a small piece of tissue, called the epiglottis, which moves to cover the larynx to prevent food from entering the air passages.
The paranasal sinuses are small hollow spaces in the bones of the head surrounding the nose. The nasal cavity is the hollow space inside the nose.
The major salivary glands are on the floor of the mouth and near the jawbone. The salivary glands produce saliva. Head
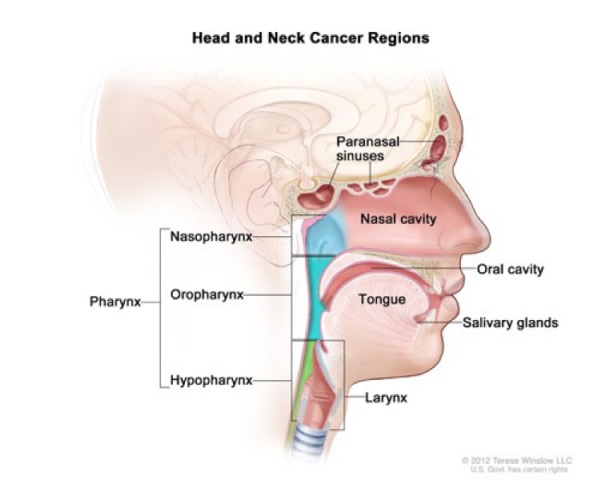
Head and neck cancer regions. Illustrates the location of paranasal sinuses, nasal cavity, oral cavity, tongue, salivary glands, larynx, and pharynx (including the nasopharynx, oropharynx, and hypopharynx).
Cancers of the brain, the eye, the esophagus, and the thyroid gland, as well as those of the scalp, skin, muscles, and bones of the head and neck, are not usually classified as head and neck cancers.
Sometimes, cancerous squamous cells can be found in the lymph nodes of the upper neck when there is no evidence of cancer in other parts of the head and neck. When this happens, the cancer is called metastatic squamous neck cancer with unknown (occult) primary.
Alcohol and tobacco use (including smokeless tobacco, sometimes called (chewing tobacco) are the two most important risk factors for head and neck cancers, especially cancers of the oral cavity, oropharynx, hypopharynx, and larynx. At least 75 percent of head and neck cancers are caused by tobacco and alcohol use. People who use both tobacco and alcohol are at greater risk of developing these cancers than people who use either tobacco or alcohol alone. Tobacco and alcohol use are not risk factors for salivary gland cancers.
Infection with cancer-causing types of human papillomavirus (HPV), especially HPV-16 and 18, are risk factors for some types of head and neck cancers, particularly oropharyngeal cancers that involve the tonsils or the base of the tongue. In the United States, the incidence of oropharyngeal cancers caused by HPV infection is increasing, while the incidence of oropharyngeal cancers related to other causes is falling. Other risk factors for cancers of the head and neck include the following: Betel nut, radiation exposure, family history, Epstein Barr virus, and occupational exposures.
The symptoms of head and neck cancers may include a lump or a sore that does not heal, a sore throat that does not go away, difficulty in swallowing, and a change or hoarseness in the voice. These symptoms may also be caused by other, less serious conditions. It is important to check with a doctor or dentist about any of these symptoms. Symptoms that may affect specific areas of the head and neck include the following:
A white or red patch on the gums, the tongue, or the lining of the mouth; a swelling of the jaw that causes dentures to fit poorly or become uncomfortable; and unusual bleeding or pain in the mouth.
Trouble breathing or speaking; pain when swallowing; pain in the neck or the throat that does not go away; frequent headaches, pain, or ringing in the ears; or trouble hearing.
Pain when swallowing or ear pain.
Sinuses that are blocked and do not clear; chronic sinus infections that do not respond to treatment with antibiotics; bleeding through the nose; frequent headaches, swelling or other trouble with the eyes; pain in the upper teeth; or problems with dentures.
Swelling under the chin or around the jawbone, numbness or paralysis of the muscles in the face, or pain in the face, the chin, or the neck that does not go away.
Avoid alcohol, tobacco, and risky exposures. This includes avoiding HPV sexual exposures and may include vaccines such as the Gardasil or Cervarix shot.
When a patient develops a lump, swelling or non-healing wound of the head and neck, he or she will typically seek medical attention. Your primary care physician will typically try medical or non-surgical therapy, such as antibiotics, to make the swelling or mass improve. If there is no significant improvement, he or she will typically refer to a head & neck surgeon for further evaluation. During that visit, you will be asked about the symptoms of timing, duration, and exposure that lead to the current findings. Then a thorough physical examination will be performed allowing for better determination of the size and severity of the lesion. The location will tell many details as to the nature of the lesion.
For example, a lump in the posterior triangle of the neck can be present in lymphoma, thyroid cancer, nasopharyngeal cancer, lipoma, cysts, lymphadenopathy from infection and melanoma. Therefore, location can aid the evaluation and diagnosis of these abnormalities. After a thorough examination, a biopsy may be required for further evaluation. This often comes in the form of a fine needle aspiration biopsy (FNAB). These biopsies are performed in the office or with ultrasound guidance and can give typically 4 answers including cancer, not cancer, atypical or insufficient. Next, imaging and laboratory studies may be required do determine the extent and spread of the lesion. Your physician will guide you through these examinations.
The treatment plan for an individual patient depends on several factors, including the exact location of the tumor, the cancer's stage, and the person's age and general health. Treatment for head and neck cancer can include surgery, radiation therapy, chemotherapy, targeted therapy, or a combination of treatments.
People who are diagnosed with HPV-positive oropharyngeal cancer may be treated differently than people with oropharyngeal cancers that are HPV-negative. Recent research has shown that patients with HPV-positive oropharyngeal tumors have a better prognosis and may do just as well on less intense treatment.
Cancers include different anatomic regions:
The patient and the doctor should consider treatment options carefully. They should discuss each type of treatment and how it might change the way the patient looks, talks eats or breathes.
Surgery for head and neck cancers often changes the patient's ability to chew, swallow, or talk. The patient may look different after surgery, and the face and neck may be swollen. The swelling usually goes away within a few weeks. However, if lymph nodes are removed, the flow of lymph in the area where they were removed may be slower and lymph could collect in the tissues, causing additional swelling; this swelling may last for a long time.
After a laryngectomy (surgery to remove the larynx) or other surgery in the neck, parts of the neck and throat may feel numb because nerves have been cut. If the lymph nodes in the neck were removed, the shoulder and neck may become weak and stiff.
Patients who receive radiation to the head and neck may experience redness, irritation, and sores in the mouth; a dry mouth or thickened saliva; difficulty in swallowing; changes in taste; or nausea. Other problems that may occur during treatment are loss of taste, which may decrease appetite and affect nutrition, and earaches (caused by the hardening of ear wax). Patients may also notice some swelling or drooping of the skin under the chin and changes in the texture of the skin. The jaw may feel stiff, and patients may not be able to open their mouth as wide as before treatment.
Regular follow-up care is very important after treatment for head and neck cancer to make sure that cancer has not returned, or that a secondary, primary or recurrent cancer has not developed. Depending on the type of cancer, medical checkups could include exams of the stoma, if one has been created, and of the mouth, neck, and throat. Regular dental exams may also be necessary. Nothing substitutes the need for physical examination and regular checkups.
From time to time, the doctor may perform a complete physical exam, blood tests, x-rays, and CT scan, PET scan, and MRI scans. The doctor may monitor laboratory levels, especially if the head or neck was treated with radiation. Also, the doctor is likely to counsel patients to stop smoking.
If you smoke, it is highly recommended you STOP SMOKING!
Comprehensive Therapy for all Disorders of the Head and Neck
3501 North Scottsdale Rd., Suite 160
Scottsdale, AZ 85251
(480) 273-8448
Copyright © 2026
Website by Red Advertising
